Wrist Joint, Basic anatomy and Biomechanics, Wrist theories,
Wrist Joint
Anatomy & Biomechanics
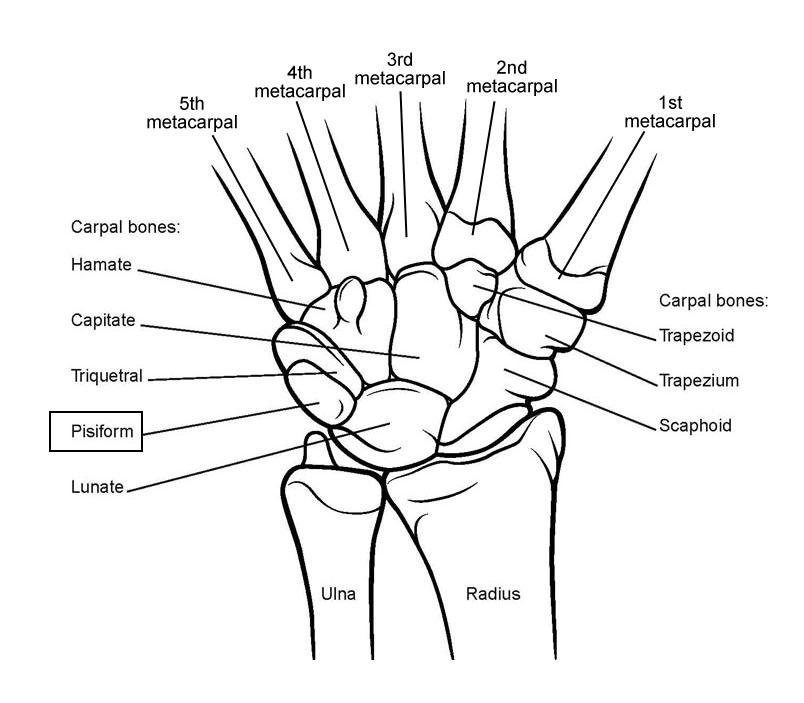
The wrist joint is a diarthrodial joint composedof two rows of carpal bones.
The proximal row articulates with the distal articular surface of the radius, which consists of the scaphoid fossa and the lunate fossa.
The distal surface of the scaphoid, lunate, and triquetrum articulate with the distal carpal row, comprised of the trapezium, trapezoid, capitates, and hamate.
The proximal articulation of the wrist is the radiocarpal joint, the distal articulation is the midcarpal joint.

Six major articulations are
Radiocarpal
Midcarpal
Pisotriquetral
Trapeziometacarpal
Common carpometacarpal
Distal radioulnar joints.
Each has multiple subarticulations.
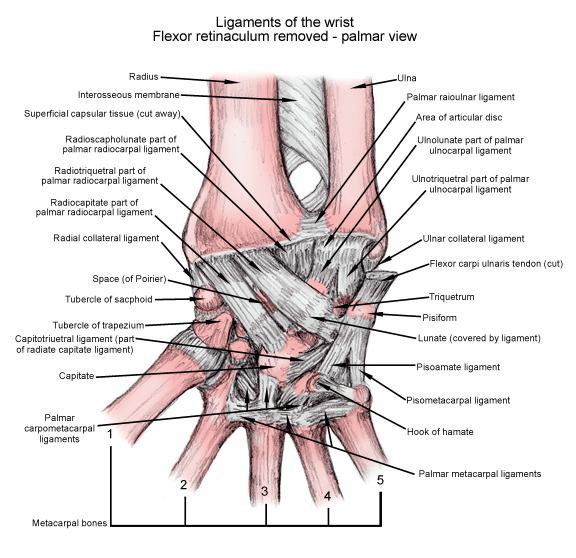
The intrinsic ligaments hold the bones of the proximal and distal carpal rows together.
Each of the carpal bones is unique in its mechanics and possesses a unique center of rotation. The overall motion in the wrist is, essence, the sum of k bones moving on each other, influenced by their articulations, ligamentous attachments, and indirect actions of adjacent tendons.
An understanding of the normal biomechanics helps in to assess the mechanisms of wrist injuries better and determine the appropriate treatment.
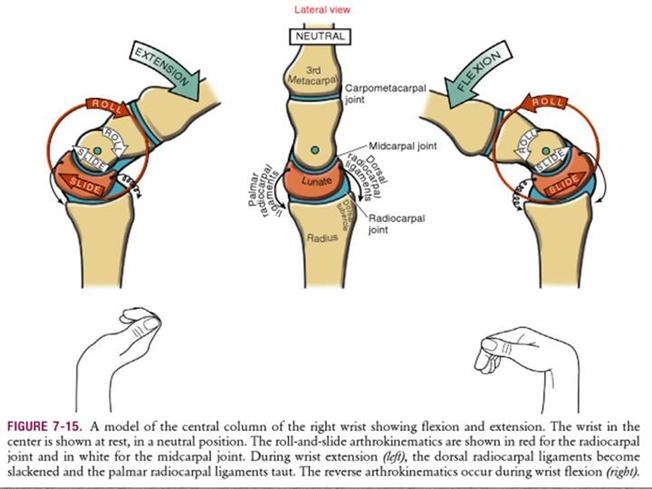
Wrist motion occurs at radiocarpal and intercarpal or midcarpal joints.


There are three axes of motion
Flexion-extension
Radial-ulnar deviation
Prono-supination
Different movements of the wrist are
Flexion is about 65-75 degrees. 40% of the movement is at radiocarpal joint and 60% is at midcarpal joint.
Extension is also about same degrees and the amount of movement contribution differs. 66% is radiocarpal and 33% is midcarpal
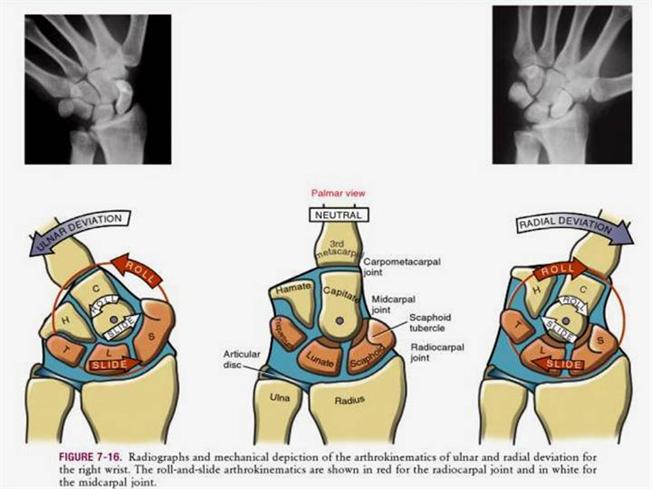
Normal radial deviation is about 15-25 degrees and 90% movement is midcarpal
Ulnar deviation is about 35-50 degrees and is equally divided in radiocarpal and midcarpal joints.
The carpus is biaxial in nature and maintains a constant carpal height ratio during radial and ulnar deviation.
[This ratio is the distance from the base of the third metacarpal to the distal subchondral plate of the radius, divided by the length of the third metacarpal. This normal carpal height ratio is 0.54+_ 0.03.]
The proximal carpal row is an intercalated segment with no tendon attachments. All the tendons that influence wrist motion insert distally, either
Base of the metacarpals
Flexor carpi radialis
Extensor carpi radialis longus and brevis
Extensor carpi ulnaris
Onto the pisiform
Flexor carpi ulnaris
Thus, wrist motion in any plane must be initiated at the distal carpal row. Motion in the proximal carpal row begins only when the extrinsic ligaments crossing the midcarpal joint become taut and the force exerted on the proximal carpal row becomes greater than the frictional forces of the intervening articular segments and the resistance of the antagonistic muscular forces.
In spite of some motion between the individual bones of the distal carpal row, these bones function as a single unit with the index and middle metacarpals.
Wrist motion produces multiplanar motion of the distal carpal row because of geometry.
During flexion of the wrist
-Distal carpal row flexes and deviates slightly ulnarly.
During extension
-the distal carpal row extends and deviates radially.
With radial deviation
-the distal carpal row deviates radially, extends and supinates.
With ulnar deviation
-The distal carpal row deviates ulnarly, flexes, and pronates
.
Thus, the relationship between the distal carpal row and the index and middle metacarpals is maintained throughout all directions and magnitudes of motion.
But the proximal carpal row cannot be considered a single functional unit as a significant motion occurs between the bones.
There is coordinated motion between the distal and proximal carpal rows.
As the distal carpal row flexes, the proximal carpal row also flexes. Similarly, when the distal carpal row extends, the proximal carpal row extends.
Radial or ulnar deviation involves a complex reciprocating motion of the proximal and distal carpal rows.
Distal carpal row inclines radially and extends and supinates whereas proximal carpal bones principally flex and translate ulnarly.
With ulnar deviation, the opposite occurs. The distal carpal row inclines ulnarly and flexes and pronates, whereas the proximal carpal bones extend and translate radially. These complex motions are required to maintain the carpal congruency and spatial consistency in all wrist positions.
The scaphoid, because of its position, has the potential energy for flexion, while the triquetrum, because of its articulation with the hamate, has potential energy for the extension. This potential energy created in the proximal carpal row is facilitated by a scapholunate interosseous ligament, which stabilizes the scaphoid and the lunate, and the lunotriquetral interosseous ligament, which stabilizes the lunate and the triquetrum.
The result is a dynamic, balanced lunate within the proximal carpal row. During radial deviation, the proximal carpal row translates toward the ulna, while the distal carpal row inclines toward the radius. Additionally, the scaphoid must flex to avoid impinging on the radial styloid, and the entire proximal row is pulled into flexion as long as there is an integrity of the scapholunate interosseous ligament.
In ulnar deviation of the carpus, the triquetrum is forced into extension by its helicoid articulation with the hamate. This pushes the remainder of the proximal carpal row into extension by virtue of the force transmission through the LTIL. in contrast, the distal carpal row has negligible intracarpal motion, being generally bound together by very short, stout ligaments with broad insertions.
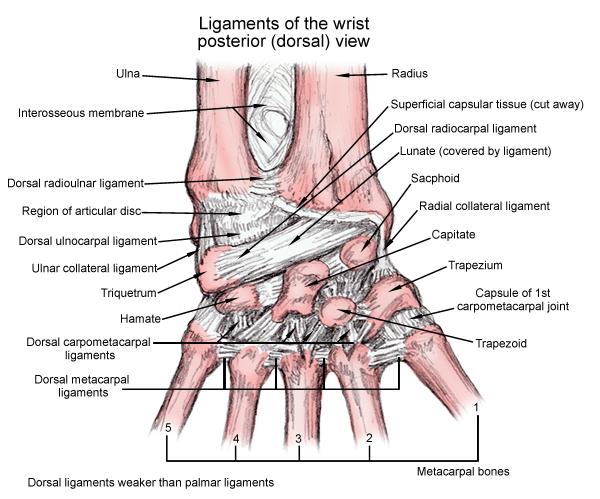
Ligaments, in general, are composed of 90% type I collagen and 10% type III collagen and function primarily as viscoelastic structures
The relatively greater strength and viscoelastic nature of the interosseous ligaments reflect their functional characteristics and anatomy. The complex, intercalated movements of the proximal carpal row are facilitated by the interosseous ligaments, which are strong and particularly accommodating to shear stress. The extrinsic wrist ligaments, by contrast, are much weaker and stiffer because there is little need for these structures to have dynamic capabilities.
In spite of knowing the movements, the principle or theory of carpal motion is not fully elucidated.
Following theories have been floated.
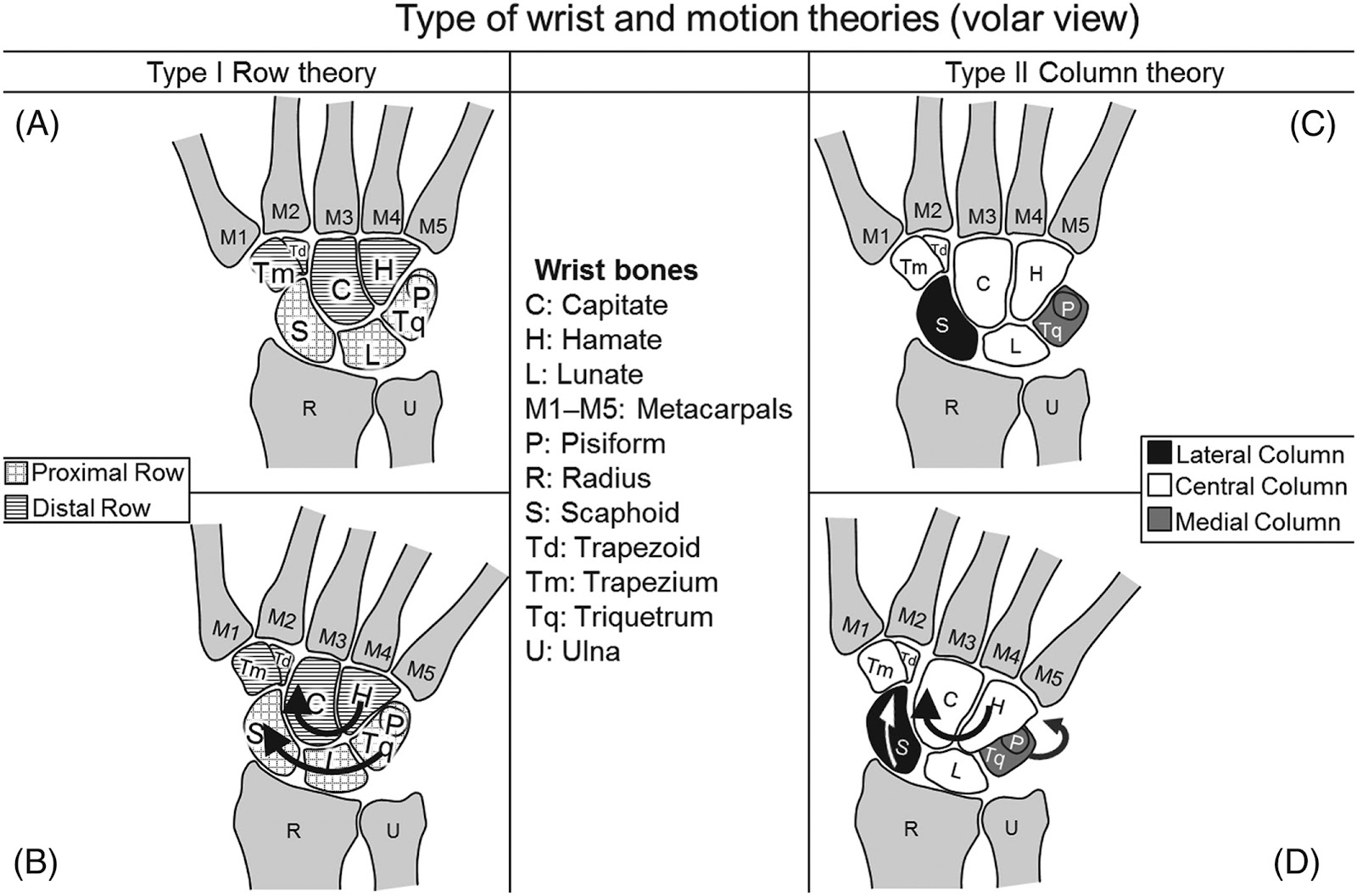
Column theory of carpal kinematics
The column theory was first proposed by Navarro in 1935. It divides the wrist into the following three columns:
Radial column, consisting of the scaphoid, the trapezium, and the trapezoid. The scaphoid is center of motion and it is mobile
Central column, including the lunate and the capitates and participate in flexion-extension motion
Ulnar column or medial column, consisting of the triquetrum and the hamate and the motion is rotation.
Row theory of carpal kinematics
Comprises proximal and distal rows
Scaphoid is a bridge between rows
Motion occurs within and between rows
Muscle contractions impart rotational moments to the proximal row through the distal row, and carpal motion is governed by a combination of ligamentous and articular constraints.
The scaphoid, lunate, and triquetrum rotate in the same primary direction, albeit to different magnitudes, during any movement of the hand.
Combined column-row theory of carpal kinematics
Some have theorized that an individual’s carpal kinematic behavior can be explained by some combination of the columnar theory with the row theory.
It is found that the amount of scaphoid shortening and ulnar translation of the scaphoid varies in a normal distribution.
Also, if the scaphoid shortens more, it translates less. Some authors attribute it to the difference in individual laxity.
In radial-ulnar deviation, the scaphoid of very lax wrists moved preferentially in the sagittal plane (flexion-extension), whereas in the more rigid wrists, the scaphoid moved preferentially in the frontal plane (radioulnar deviation).
Oval-ring theory of carpal kinematics
The oval-ring theory functionally depicts the carpus as a transverse ring formed by proximal and distal rows and joined by two physiologic links, one radial and the other ulnar.
The radial link is the mobile scaphotrapezial joint, and the ulnar link is the rotatory triquetrohamate joint.

Mechanism of Wrist Injuries
Radial-Sided Carpal Instabilities
These occur following injury caused by compressive force across a hyperdorsiflexed wrist.
The spectrum of injuries has a common mechanism
Hyperdorsiflexion of the wrist
Forearm pronation
Ulnar deviation of the hand
Axial loading of the wrist through the radial palm and thenar eminence
Four distinct Patterns of injury are collectively called progressive perilunate instability.
That progression occurs in four stages.
Stage I
Disruption of the scapholunate and radioscaphocapitate ligament
Stage II
The capitates and scaphoid separate from the lunate and the triquetrum.
Stage III
Injury continues ulnarly and separates the triquetrum from the lunate. Carpus is completely separated from the lunate resulting in a perilunate dislocation.
Stage IV
Complete lunate dislocation. The perilunate and the lunate dislocations may occur in a dorsal or palmar direction.
Pure perilunate dislocation, without fractures, is termed lesser arc injury.
Perilunate dislocations with fractures are called t greater arc injuries and are prefixed with trans. The pure greater arc injury propagates in a tran-scaphiod, transcapitate, and trans-triquetral fashion. Typically, these injuries occur secondary to high-energy trauma, and the position of the wrist at the time of injury will determine the fracture-dislocation pattern
They are thought to result from high-energy three-dimensional loading of the wrist with axial and torsional forces applied to any combination of hyperextension, hyperflexion, and radial or ulnar deviation.
Ulnar-Sided Wrist Ligament Injuries
Some perilunate wrist injuries initiate on the ulnar side of the wrist.
These are lunotriquetral ligament injuries along with a spectrum, beginning with simple ligament tears and progressing to static ventral intercalated segment instability.
Progressive perilunate disruption is a three-stage injury mechanism.
Stage I
Tear of the lunotriquetral ligament
Stage II
Disruption of the palmar ulnar leash complex
Dorsal radiotriquetral and the dorsal scaphotriquetral ligaments
Stage III
Tear of the scapholunate ligament
Axial Disruptions
[Also longitudinal disruption capitohamate diastasis and columnar dislocations.]
Axial disruption of the wrist are and usually occur secondary to high-energy crush or blast injuries as derangement of the carpus that is oriented parallel to the long axis of the forearm.
In axial carpal disruption, the normal convexity of the metacarpal arch is flattened, rotational deformities of the fingers occur, and the carpometacarpal junction is widened.
The typical mechanism of the injury of axial carpal disruptions a crush[most common], twisting, or blast injury.
The spectrum ranges from acute traumatic fracture dislocations with severe soft-tissue trauma to chronic dynamic instability between the axial components.
Three groups have been defined according to the direction of the instability
Axial-ulnar disruptions
Axial-radial disruptions
Combined axial-radial-ulnar disruptions.
In axial-ulnar disruptions, the carpus splits into two columns, with the radial column stable with respect to the radius and the ulnar column with the metacarpals is displaced ulnarly and proximally.
In axial-radius disruptions, the ulnar column is stable with respect to the radius, and the radial column including the metacarpals displaces proximally and radially.
A combination of the ulnar and radial displacement of the column is classified as an axial-radial-ulnar disruption.


Comments
Post a Comment