Gait Patterns, Ambulation Phase, cane, crutches, walker...
Gait Patterns
There are two types of gait patterns described in crutch walking:
a. Based on the type of step taken Here two types are described step-to or step-through.
b. Based on the number of contact points used to take a step
Here three types are described 2 point, 3 point and 4 point gaits.
Now let us analyse each step in detail:
1. Step-to-gait In this the crutch and the fractured limb are advanced first and then the normal limb is advanced to the same position. E.g. Partial weight bearing or toe touch weight bearing after a tibial shaft fracture.
2. Swing through gait Here the intact leg is advanced first with the crutch and then the fractured leg is advanced towards it. E.g. oblique mid-shaft tibial fracture that is non weight bearing practices this gait (see Figs 1.18A and B).

3. A two point gait (Fig. 1.19A)
• One point is formed by the fractured leg and crutches.
• Second unit by the uninvolved leg.
In this gait, the second unit is brought towards the first unit. e.g. A NWB fracture of femur.
4. A three point gait
• First point—formed by the crutches.
• Second point—involved leg.
• Third point—uninvolved leg.
In this, each crutch and the weight limb are advanced separately, with two of the three points touching the ground at any given point of time. E.g. In femoral neck fracture that are partially weight bearing. Here the crutches are advanced first, followed by the fractured and intact limb respectively (Fig. 1.19B).
5. Four point gait
Point No 1 This is the crutch on the involved side.
Point No 2 This is the uninvolved leg.
Point No 3 The involved leg.
Point No 4 Crutch on the uninvolved side.
Here the crutches and the limbs are advanced separately. With three of the four points touching the ground at any given time. E.g. a partially weight bearing fracture with an additional problem like muscle weakness, anxiety, etc. (Fig. 1.19C

Crutch Walking in Special Situations
1. Walking on uneven surfaces like staircases
• Ascend the staircase with the unaffected leg first.
• Then bring the fractured limb up to meet the first leg, either simultaneously with the crutches or by keeping the crutches on the step below until both the feet are level.
• While descending the stairs, the reverse is done and fractured limb is brought down first.
2. Getting in and out of a chair The chair should be well supported to prevent it from slipping. Remove the crutches from under one arm thereby freeing it.
Now with the freed hand, the patient pushes down on the chair set or armrest to support the body weight.
Finally the patient gradually sits by flexing the elbow.
The reverse technique is used while getting up from the chair.
3. Climbing staircases with support (bannister) Hold one or two crutches on the uninvolved side. Hold the bannister with the hands on the side of fracture. Climb the staircase first with the uninvolved leg then pull the body up to bring the affected leg on the same point as the unaffected leg.
The opposite is followed to descend down the staircase with bannister.
Quick facts
Weight-bearing status in a lower limb fractures
• Non-weight-bearing (NWB)
• Toe-touch weight-bearing (TTWB)
• Partial weight-bearing (PWB)
• Weight-bearing as tolerated (WBAT)
• Full weight-bearing (FWB)
Shadow Walking
This is a non-weight-bearing gait—Here
• The crutch on the opposite side of NWB is put forward first.
• The non-weight bearing limb is advanced next.
• The second crutch is put forward next.
• This is followed by the advancement of the normal limb.
Ambulation with the Help of a Cane
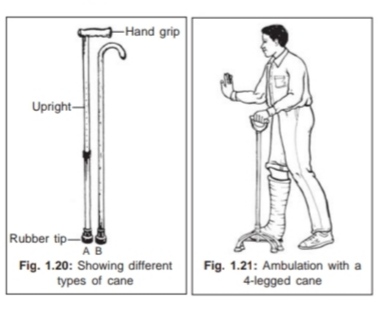
Purpose of a cane To relieve one extremity of some weight bearing load. This also provides continuous stability to the patient (Fig. 1.20).
Types of cane
1. Standard cane
2. Axillary crutch can be used like a cane
3. Three or four legged cane can be used by the elderly.
This provides greater stability (Fig. 1.21)
4. Hemi walker: Patient uses this walker like a cane by holding it on the opposite side.
Parts of a cane
• Hand grip
• An upright
• Bottom with a rubber tip.
• It is made up of either aluminium or wood.
Methods of walking with a cane
• The patient stands holding the wall or chair for support.
• The heel of the shoes should be about 1-1½”.
• The height of the cane should be such that, the elbow is flexed to 25-30°.
• The patient is instructed to hold the cane on the unaffected side.
• Patient is advised to take short steps.
Quick facts
Why should the patient, hold the cane on the unaffected side:
1. In normal walking the leg and opposite arm move together.
2. It increases stability by providing a wider base.
3. The shifting of the centre of gravity is eliminated.

Comments
Post a Comment